Millions of dollars are left on the table every year because of billing errors, delayed claims, and poor documentation practices. The good news? Most of these losses are preventable, and the right process improvements can transform your revenue cycle starting today.
Why the Medical Billing Process Matters More Than Ever
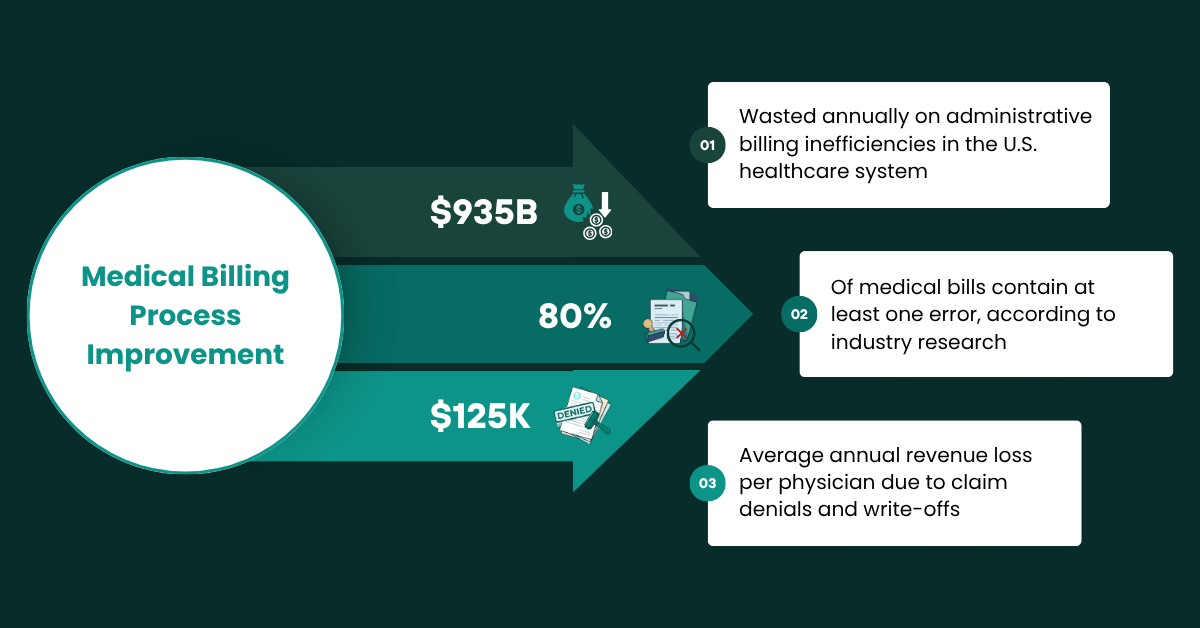
The financial health of any medical practice is directly tied to the efficiency of its billing process. When claims are submitted with errors, when documentation is incomplete, or when follow-ups on denials are delayed revenue suffers. Patients are billed incorrectly. Staff are overwhelmed. And providers are left wondering why their actual collections never seem to match what was expected.
The medical billing process has grown more complex over the past decade. Between ICD-10 code expansions, shifting payer requirements, telehealth regulations, and value-based care transitions, it’s no surprise that most practices large and small struggle to maintain a clean revenue cycle. According to the CAQH Index Report, billions in administrative costs could be eliminated simply by moving to fully electronic billing and eligibility processes.
Yet many practices still rely on fragmented, manual workflows. And that’s where the gap between earned and collected revenue begins to widen.
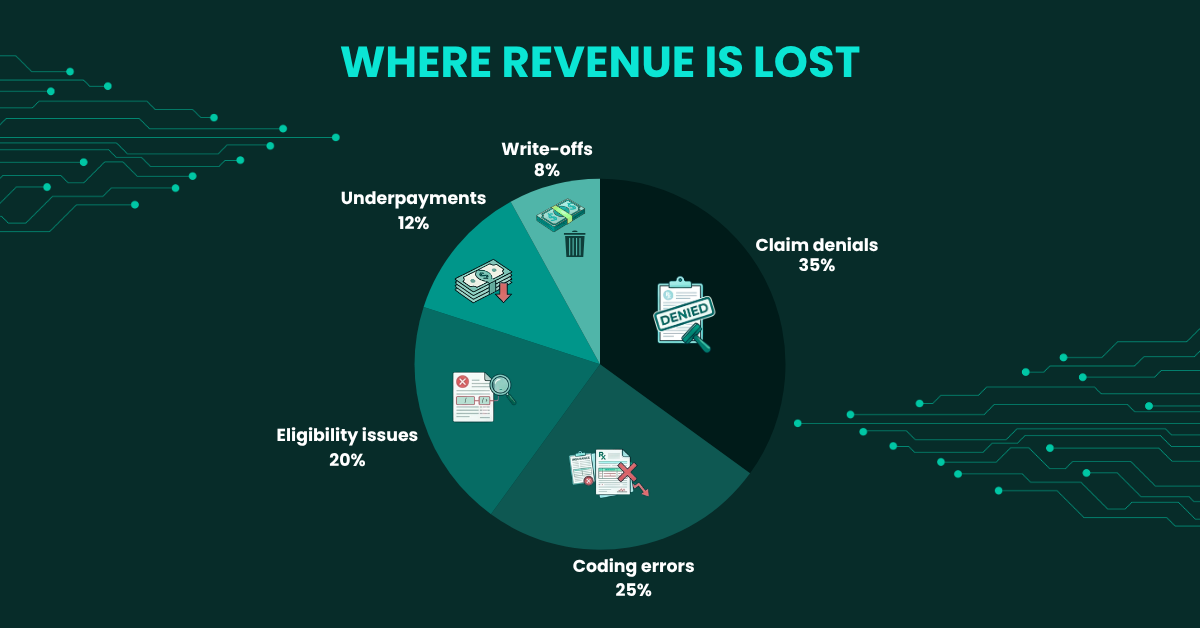
Only 56% of denied claims are ever resubmitted — meaning practices routinely write off revenue that could realistically be recovered with a proper denial management system in place. That represents an enormous, silent drain on practice income.
Common Medical Billing Errors and Their Real Cost
Billing errors aren’t always caused by negligence. In many cases, they’re the result of outdated systems, undertrained staff, or processes that simply haven’t kept pace with payer requirements. Understanding the most common errors is the first step toward eliminating them.
| Error Type | Description | Financial Impact | Frequency |
|---|---|---|---|
| Incorrect Patient Information | Wrong DOB, insurance ID, or address on the claim | Immediate denial — resubmission delays of 30–60 days | Very High |
| Upcoding / Downcoding | Services billed at incorrect code levels | Revenue loss or compliance penalties up to $11,000/claim | High |
| Duplicate Billing | Same service billed more than once | Payer audit flags, clawbacks, and legal risk | Moderate |
| Missing Prior Authorization | Services rendered without required payer pre-approval | Full denial (often non-recoverable) | High |
| Unbundling | Billing separately for procedures that should be bundled | Audits, refund demands, exclusion from payer networks | Moderate |
| Incorrect Modifier Use | Wrong or missing CPT modifiers applied to claims | Partial or full denial; manual review delays | Very High |
| Timely Filing Violations | Claims submitted after payer deadline windows | Permanent revenue loss — no appeal option | Low–Moderate |
A 12-physician orthopedic group in Ohio had been experiencing a steady 22% claim denial rate for over 18 months. After an internal audit was conducted by their billing manager, the root cause was traced to the inconsistent use of CPT modifier -59 across three providers. No standardized modifier guide had been distributed since 2021. Insurance contracts were also reviewed and it was discovered that two major payers had updated their bundling rules, changes that had never been applied to their billing system.
✅ Outcome: After standardization training and a modifier audit, their denial rate dropped to 8.4% within 90 days, recovering approximately $310,000 in previously denied claims.
The Ideal Medical Billing Workflow: Step by Step

Leveraging Technology to Streamline Billing
Technology has transformed what’s possible in revenue cycle management. From AI-powered claim scrubbing to automated eligibility verification, the right tools can dramatically reduce manual effort and error rates. But technology only works when it’s implemented correctly and used consistently.
Electronic Health Records (EHR) Integration
When EHR and billing systems are properly integrated, clinical documentation is automatically translated into billing codes, removing one of the most error-prone manual steps in the process. According to Health Affairs, practices with tightly integrated EHR-billing workflows report up to 30% fewer coding errors and significantly faster reimbursement timelines.
Automated Eligibility Verification
One of the simplest and most impactful upgrades a practice can make is implementing real-time insurance eligibility checks. When verification is run at the time of scheduling not just at check-in the number of denials tied to coverage issues falls dramatically. Most modern practice management systems offer automated batch verification for upcoming appointments.
Eligibility-related denials account for nearly 24% of all first-pass claim rejections making it the single largest preventable category of denials. Yet fewer than 40% of practices verify eligibility more than 24 hours before a patient’s visit.
AI-Powered Claim Scrubbing
Modern claim scrubbing software, particularly systems powered by machine learning, can identify coding issues, missing information, and payer-specific rule violations before a claim is ever submitted. These tools learn from historical denial patterns and flag high-risk claims automatically. The result is a higher first-pass claim rate and fewer resources spent on rework.
❌ Without Automated Tools
- Manual eligibility checks at check-in only
- Coding reviewed only after claim denial
- Spreadsheets used to track denials
- Billing staff manually reviewing every claim
- Days in AR often exceed 45–60 days
- Limited visibility into denial trends
✅With Optimized Technology
- Automated eligibility at scheduling & check-in
- Real-time claim scrubbing before submission
- Denial dashboard with root cause tagging
- AI flags high-risk claims for review
- Days in AR reduced to 25–35 days
- Monthly trend reports generated automatically
Denial Management: Turning Rejections into Revenue
Denial management is where revenue cycle improvement delivers some of its most immediate and measurable results. A well-structured denial management process doesn’t just recover lost claims, it identifies the systemic issues that caused those denials in the first place, preventing future losses at their source.
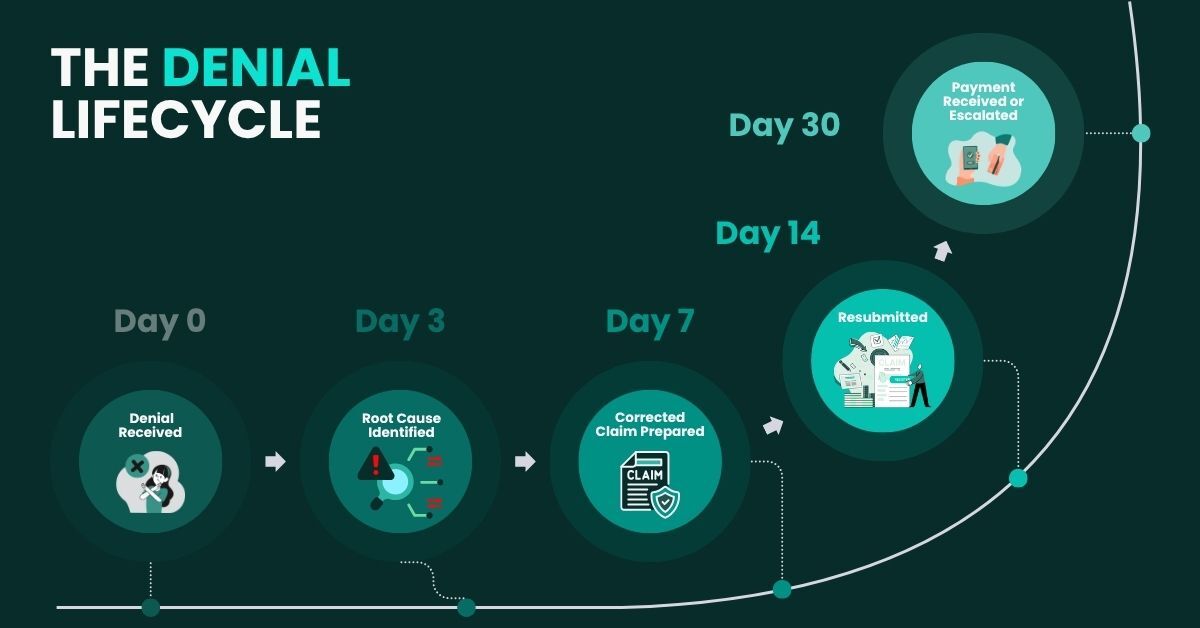
A 6-physician family medicine practice was writing off an average of $18,000 per month in denied claims. After a denial management review was implemented, including a 30-day rolling denial report and a weekly team review meeting, it was discovered that 61% of denials were related to just two payers. A payer-specific billing protocol was developed for both. Simultaneously, authorization tracking was moved into their EHR instead of a separate spreadsheet.
✅ Outcome: Monthly write-offs dropped from $18,000 to $4,200 within 60 days. Annual revenue recovery: approximately $166,000.
Accurate Medical Coding: The Foundation of Clean Claims
Every claim begins with a code. And when that code is inaccurate, even by one digit, the entire claim can be denied, delayed, or flagged for audit. Medical coding accuracy is non-negotiable, yet it remains one of the most undertrained areas in many practices.
“Accurate coding is not just a billing issue; it is a clinical documentation issue. The two cannot be treated separately.”
— AAPC (American Academy of Professional Coders) AAPC Coder Resources
ICD-10 Specificity
With over 70,000 diagnostic codes in ICD-10-CM, the expectation is that clinical conditions are coded with maximum specificity. Unspecified codes, while sometimes unavoidable, are frequently targeted by payers for additional documentation requests or automatic denials. Physicians and coders should be aligned on the level of detail required in clinical notes to support specific code selection.
Annual Code Updates
ICD-10 codes are updated every October 1, and CPT codes are updated each January. Most practices acknowledge these updates, but fewer than half have a documented process for training staff and updating their systems before the effective date. As a result, outdated codes are submitted, claims are rejected, and valuable time is lost to rework. Learn more about staying current via the CMS Coding & Billing Resources.
Upcoding, even when unintentional, can trigger a False Claims Act investigation under federal law. Annual coding audits are strongly recommended for every practice, regardless of size. Internal audits should be conducted quarterly at a minimum.
Compliance, Audits, and the Risks of Getting it Wrong
Billing compliance isn’t just about staying out of trouble — it’s about building a practice that payers trust and patients respect. Non-compliant billing practices carry consequences that extend far beyond individual claim denials: OIG investigations, Medicare exclusion, and civil monetary penalties are all realistic outcomes of systemic billing problems.
| Compliance Risk Area | Governing Body | Potential Penalty | Risk Level |
|---|---|---|---|
| False Claims Act Violations | DOJ / OIG | $13,946–$27,894 per claim + 3x damages | Critical |
| HIPAA Billing Data Breaches | HHS OCR | Up to $1.9M per violation category | Critical |
| Anti-Kickback Violations | OIG | $50,000 per violation + exclusion | High |
| Stark Law (Self-Referral) | CMS | Up to $15,000 per prohibited service | High |
| Medicare Advantage Audits (RADV) | CMS | Recoupment of overpayments + interest | Moderate–High |
Key Metrics Every Billing Team Should Track
What isn’t measured can’t be improved. The highest-performing revenue cycle teams are data-driven they monitor a core set of KPIs on a weekly or monthly basis and take action when metrics fall outside acceptable ranges.
Industry Benchmark vs. Common Practice Performance
How most practices compare to top-quartile benchmarks across key billing metrics
Source: MGMA DataDive 2025; HFMA Revenue Cycle Metrics Benchmarking Report
Practices that track and review billing KPIs on a weekly basis, rather than monthly or quarterly report 23% higher collection rates and resolve claim denials an average of 11 days faster than those who review metrics less frequently.
Cardiology Practice, New York: KPI-Driven Turnaround
A high-volume cardiology group with 9 providers had never formally tracked Days in AR as a practice KPI. Their billing manager was reporting collections on a monthly basis, but no one was monitoring aging buckets. After a revenue cycle consultant was brought in, it was discovered that $2.1M in claims were sitting in the 90–120+ day aging bucket, with no active follow-up assigned. A structured AR follow-up protocol was implemented, with daily task queues generated for the billing team based on payer, age, and value.
✅ Outcome: $1.4M was recovered over 6 months. Days in AR dropped from 58 to 31. The practice now reviews AR aging every Thursday in a 20-minute billing huddle.
Conclusion:
At the end of the day, medical billing isn’t just a back-office function, it’s the financial engine of your entire practice. When your processes are tight, your coding is accurate, and your follow-ups are disciplined, revenue flows the way it should. When they’re not, even small inefficiencies quietly chip away at your bottom line.
The upside? Every gap in your billing process is an opportunity. With the right workflow, smarter use of technology, and a proactive approach to denials and compliance, you’re not just fixing problems, you’re building a revenue system that scales with your practice.
Vigilant’s revenue cycle specialists offer a free, no-obligation billing audit for qualified practices. Discover exactly where money is being left on the table — and how to get it back.
Request Your Free Billing Audit Explore Our Services