Medical billing is a world of form-filled, coding, and paper work that is something that most individuals never consider before until a claim is rejected or a reimbursement is lost. The superbill is a special document in the paperwork that passes through any healthcare practice. In various aspects, it is the beginning of the whole billing procedure.
Regardless of whether one has been treated by an out-of-network therapist, a chiropractor, or a specialist, there is a high probability that a superbill was given to him or her at the end of the visit. Knowing what is in this document, why it exists and how it is being used may save patients and providers a lot of time and money.
This blog covers everything worth knowing about superbills in the realm of medical billing.
What Is a Superbill?
A superbill is not a bill per se. It can best be termed as a very detailed receipt. It is a formatted document that summarizes all that occurred at the time of a patient visit in a format that can be read and acted upon by insurance companies.
Also known as a charge slip, encounter form or a fee ticket, a superbill has the details of the patient, the credentials of the provider, the date of the service, the diagnosis codes (ICD-10) and the procedure codes or CPT codes that explain exactly what was performed. All this information is put into one document which can be submitted to an insurance company by the patient or the provider, requesting reimbursement.
The key difference between a superbill and a regular invoice is that medical codes are included. In the absence of ICD-10 diagnosis code and CPT procedure code, an insurance company cannot review a claim. Superbill will fill this gap, making a clinical encounter a billing-ready document.
According to industry estimates, patients lose more than $50 billion annually due to improperly filed superbills. This is a number that reflects just how important accuracy in this document really is.
Key Features of a Superbill
Every well-prepared superbill should contain the following sections:
Provider Information
This section identifies the healthcare professional who rendered care. It typically includes:
- Full name of the provider
- National Provider Identifier (NPI) a 10-digit number assigned by CMS
- Practice name and address
- Phone number and email
- Referring physician’s name and NPI (if applicable)
- Provider’s signature
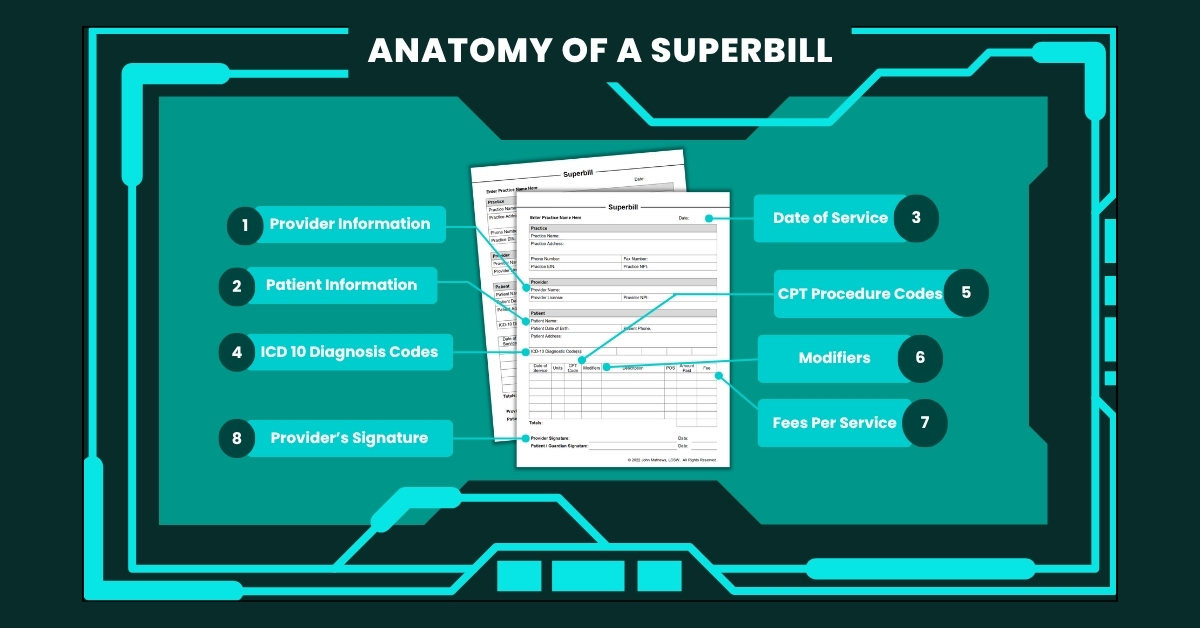
Patient Information
Accurate patient data is essential for claim matching. This section includes:
- Full legal name and date of birth
- Home address and phone number
- Insurance policy number and group number
- Insurance company name and payer ID
Visit Details
This is the most technically complex section and the most important for claim approval:
- Date of service
- ICD-10 diagnosis codes. These standardized codes are from the WHO that describe the patient’s condition
- CPT procedure codes. These codes are maintained by the AMA that describe what was done
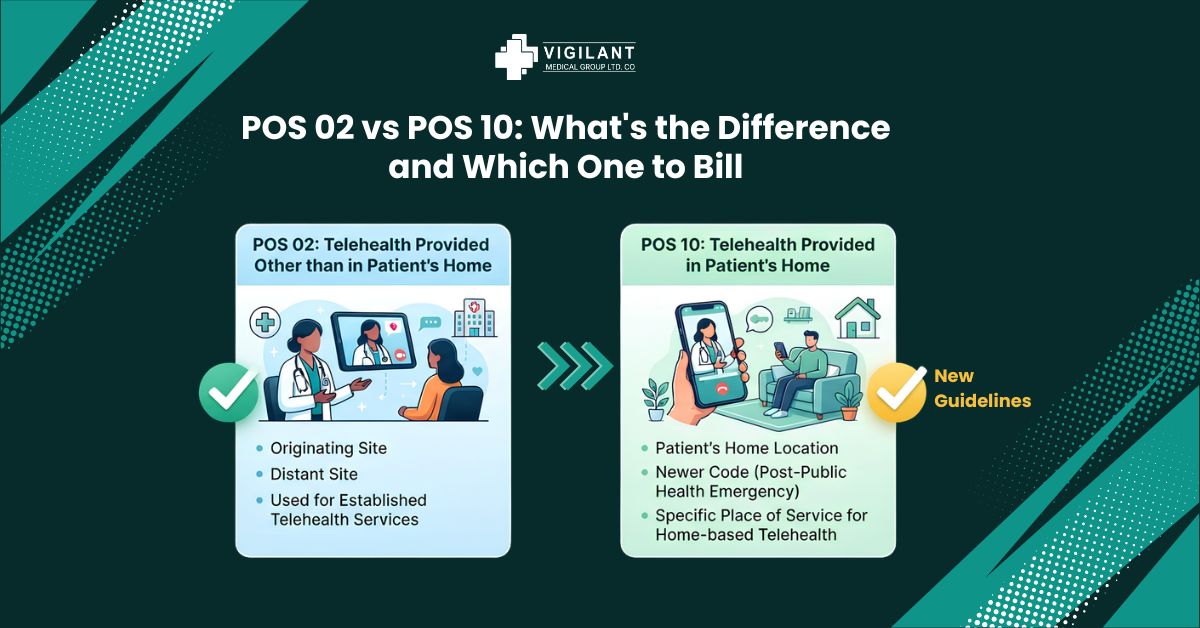
- Modifiers. These two-digit codes add context to a CPT code (e.g., telehealth delivery, bilateral procedure)
- Units or time spent (particularly relevant in therapy billing)
- Fee charged for each service
- Patient signature (where required)
How a Superbill Works in Practice
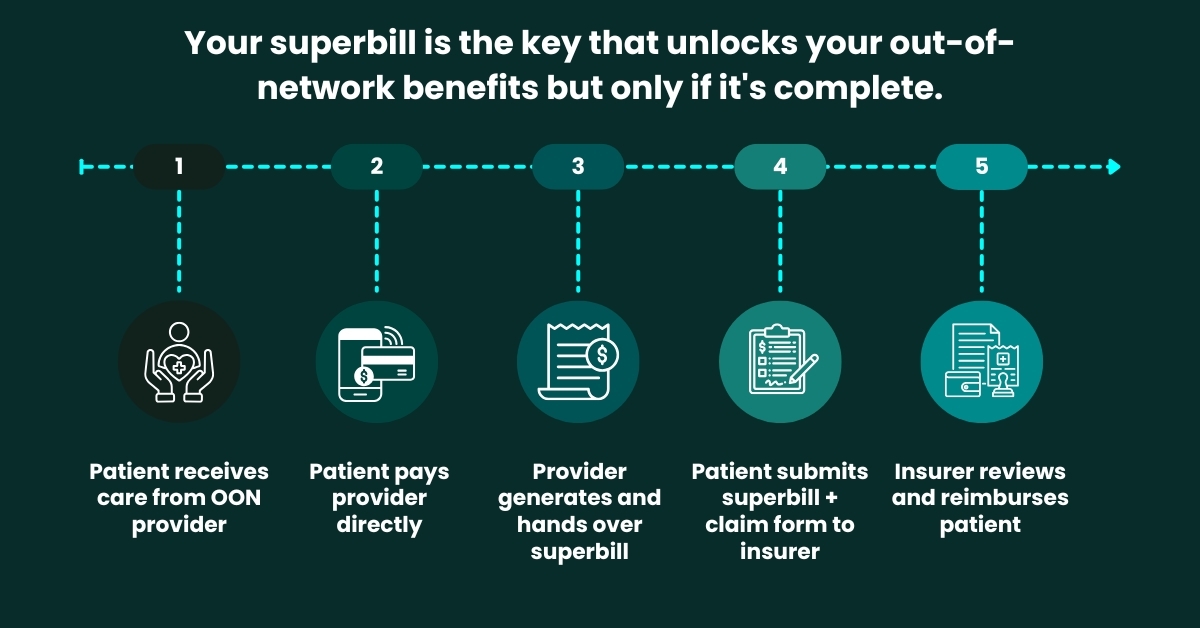
The process is straightforward, but each step matters. Here is a typical workflow for an out-of-network visit:
Step 1: The patient is cared for by an out-of-network provider.
Step 2: Payment is collected upfront by the provider directly from the patient.
Step 3: The provider office creates a superbill, which is in paper form or through EHR software.
Step 4: The patient will file the superbill to their insurance company with a claim form.
Step 5: The insurer reads the claim and upon approval, they pay the patient a part of the cost that is covered.
The provider also can file the superbill on the behalf of the patient using an electronic portal, also known as an e-superbill, in certain practices. This method minimizes the possibility of patient error in submission and normally leads to quicker processing.
Types of Superbills
Superbills can be broadly grouped into two categories based on who handles submission:
Client-Submitted Superbills:
These are prepared by the provider but handed to the patient, who then submits them independently to the insurance company. This is the most common arrangement for out-of-network care. The provider’s responsibility ends at handing over a complete and accurate document.
Provider-Submitted Superbills:
In this model, the provider’s billing team submits the superbill directly to the insurance company on behalf of the patient. This is more common in larger practices with dedicated billing staff and results in fewer submission errors.
Within these categories, specialty variations also exist. Therapy superbills must include session duration, while chiropractic superbills often note the region treated. These specialty-specific fields help insurers assess claims without requesting additional documentation.
All the codes listed in a superbill must be cross-referenced to current year CPT and ICD-10 code sets before a patient is issued with a superbill. The two sets are updated yearly. CPT according to the AMA (usually effective January 1), and ICD-10 according to the WHO (usually effective October 1).
Annual reminders of the billing calendar of both update cycles, as well as a review of any common codes used in the practice, can avoid much of the claim denials before a single form has been submitted.
Superbill vs. CMS-1500 Form
Healthcare providers use both superbills and CMS-1500 forms, but these documents serve different purposes and flow through the system differently. The table below clarifies the most important distinctions:
| Feature | Superbill | CMS-1500 Form |
|---|---|---|
| Purpose | Detailed patient receipt for reimbursement | Standard claim form submitted to payers |
| Who Submits | Patient (or provider on their behalf) | Provider / billing staff directly |
| Payment Goes To | Patient (reimbursed after payment) | Provider (direct payment) |
| Typical Use | Out-of-network care | In-network insurance billing |
| Format | Practice-specific template | Standardized government form |
| Required Codes | CPT + ICD-10 + Modifiers | CPT + ICD-10 + Modifiers + Box fields |
| Insurance Submission | Submitted by patient to insurer | Submitted by provider to payer |
| EHR Integration | Often generated automatically | Generated via billing software / clearinghouse |
| Claim Denial Risk | Higher if codes or info are incomplete | Lower when submitted via clearinghouse |
The Key Takeaway:
A superbill is used when the patient pays first and seeks reimbursement afterward, while a CMS-1500 form is used when the provider bills the insurance company directly. Both require the same core codes, but the submission path and who receives the payment is different.
Top Reasons Superbills Get Denied
Nearly 15% of all medical claims are initially denied by payers. The chart below shows the most common reasons superbill-based claims are rejected, based on analysis of industry billing data:
| Denial Reason | Frequency (% of denials) | % |
|---|---|---|
| Wrong/Outdated Codes |
|
35% |
| Missing Information |
|
28% |
| Code Mismatches |
|
18% |
| Missing Modifiers |
|
12% |
| Incomplete Provider Info |
|
7% |
Source: Industry billing data analysis, 2024–2025
Wrong or outdated codes account for the largest share of denials. CPT codes are updated every year by the AMA, and ICD-10 codes are revised annually by the WHO. A code that was valid in 2022 may have been deleted by 2024. Resubmission after a rejection of this type typically delays payment by 30 to 60 days. All of which is avoidable with up-to-date coding practices.
Why Superbills Matter for Patients and Providers
For patients, a superbill is often the only document available for accessing out-of-network insurance benefits. After the deductible is met, some insurance plans reimburse up to 80% of out-of-network service costs, but only if the claim is submitted with a complete superbill. Many patients leave this money unclaimed simply because they are unaware of how to use the document they were given.
For providers, superbills offer a path to receiving payment without the administrative burden of dealing directly with insurance companies. No pre-authorizations, no network agreements, no billing staff spending hours on hold with payer representatives. The provider collects payment directly from the patient and hands over a document and the patient handles the rest.
From a compliance perspective, superbills also serve as a legal record of the services provided. They are tied to specific dates of service and authenticated by the provider’s signature, making them traceable and auditable in the event of an insurance dispute.
Common Mistakes That Lead to Claim Denials
Most revenue cycle problems do not start with large billing errors. They start with small oversights, a blank field on a busy day, a code that has not been updated, or a modifier that was simply forgotten. Here are the most frequent mistakes found on superbills:
- Using deleted or outdated CPT or ICD-10 codes from prior years
- Mismatched code pairs (e.g., a procedure code that does not align with the diagnosis code)
- Missing or incorrect NPI number for the rendering provider
- Omitting the date of service or using an incorrect date
- Leaving the modifier blank when telehealth or bilateral procedures were involved
- Incorrect or missing patient insurance ID or group number
- No provider signature or credentials listed
- Using the ICD-9 coding system instead of the current ICD-10 standard
Each of these errors, though seemingly minor, can cause an insurer’s automated system to reject the claim outright. With no human review and no immediate explanation. The correction and resubmission process can take weeks, affecting cash flow for the provider and leaving patients without reimbursements they are entitled to.
Nearly 15% of all medical claims submitted to payers are initially denied. Of those, more than half are eventually overturned and paid. This means that the majority of initial denials are for claims that were legitimate all along.
For hospitals and health systems, appealing each of those denied claims costs an average of $43.84 per claim. A clean, accurate superbill is one of the most effective tools for keeping that cost at zero.
Frequently Asked Questions (FAQs)
What is the difference between a superbill and a regular invoice?
A: A standard invoice just enumerates. expenses. A superbill contains standard medical codes (CPT and ICD-10) which must be assessed and accepted by the insurance to claim.
Who makes a superbill?
A: It is the liability of the healthcare provider or their billing team. With bigger practices, a certified medical coder usually checks and completes the superbill and then gives it to the patient.
Is it possible to submit a superbill with in-network providers?
A: Superbills are the most typical with care out of network. In-network providers usually charge insurers a direct bill via a CMS-1500 form or its electronic counterpart.
How much time does it take to be reimbursed upon submitting a superbill?
A: The timeframes of the reimbursement are different depending on the insurer, yet a clean superbill usually leads to the processing in 30-45 days. Mistakes or unreported data can add a lot of time to that time frame.
What will occur when a superbill is rejected?
A: It is possible to rectify the claim and resubmit it. The cause of rejection is usually communicated by the insurer via an Explanation of Benefits (EOB) or a denial letter. The norm involves fixing the mistake and re-submission of the work.
Partner with Vigilant Billing Because Your Revenue Deserves It
A superbill is only as powerful as the accuracy behind it. When almost every seventh claim is denied at first, it is not a luxury, but a necessity to have a billing partner who is aware of all the fields, all the codes, and all the deadlines.
Vigilant Billing is a medical billing and revenue cycle management company that focuses on practices of any size. The team manages all claims submitted on your behalf, whether it’s superbill creation and review or full-cycle claims management, making sure that all claims are clean, compliant and coded properly.
- One of the most common reasons for reimbursements delays and claim denials is inaccurate superbills. At Vigilant Billing, a dedicated team of qualified medical billing experts are committed to ensuring that every superbill you present is clean, compliant and correctly coded the first time.