Introduction:
The term HCC is often mentioned in references to Medicare reimbursement, risk adjustment, or value-based care, and its there’s for good reason. Hierarchical Condition Categories, commonly called HCCs, sit at the heart of how Medicare determines how much it should pay to care for its beneficiaries.
If the coding is comprehensive and accurate, then the provider can be fairly compensated for HCC coding. If it is not collected or goes undocumented, revenue sneaks out the back door without anyone noticing and patients report to their health care providers with incomplete records of their health.
Vigilant Medical Group explains everything you need to know about HCC coding, including what it is, how it functions, what conditions are included and what’s a common mistake to look out for.
1. What Does HCC Stand For?
The term HCCs stands for Hierarchical Condition Category. It is a risk adjustment model developed by the Centers for Medicare & Medicaid Services (CMS). It is used to predict the healthcare costs of an individual Medicare patient.
Instead of paying a flat rate to every Medicare Advantage or Medicare Part D enrollee, CMS makes an adjustment to the payments based on patient’s actual illness using HCC coding. Patients with more complex, chronic conditions are expected to need more care, and the payment model is designed to reflect that.
The CMS Risk Adjustment Page provides the baseline information about HCC, including how the model is maintained and updated every year.
There are over 9,500 ICD-10-CM diagnosis codes, but only about 9,000 of them map to one of the 86 HCC categories used in the CMS-HCC model. Knowing which diagnoses carry HCC weight is what separates efficient coding from missed revenue
2. Why HCC Coding is Important in Medical Billing?
The importance of HCC coding has to do with its link to clinical documentation and payment. Traditional fee-for-service Medicare involves providers’ billing for services rendered. Medicare Advantage and risk-based contracts pay insurers a flat rate each month per member, with the rate being raised or lowered depending on the member’s risk score.
If the patient’s chronic conditions are properly documented and coded then their risk score increases, and the health plan receives more funding for the patient’s expected care. Providers who enter into value-based arrangements have a direct benefit from accurate HCC capture because it impacts shared savings, quality bonuses, and care coordination funding.
- Accurate HCC coding leads to proper reimbursement of complex patient panels.
- It helps in the provision of suitable care planning and resource allocation
- It helps to ensure that providers are protected during audits, having a defensible documentation trail.
- It enhances population health data analysis in the practice
HCC coding is not a one-and-done activity. Every chronic condition must be documented and coded at least once per calendar year for it to count in the annual risk adjustment submission. A diagnosis from last year does not carry forward automatically
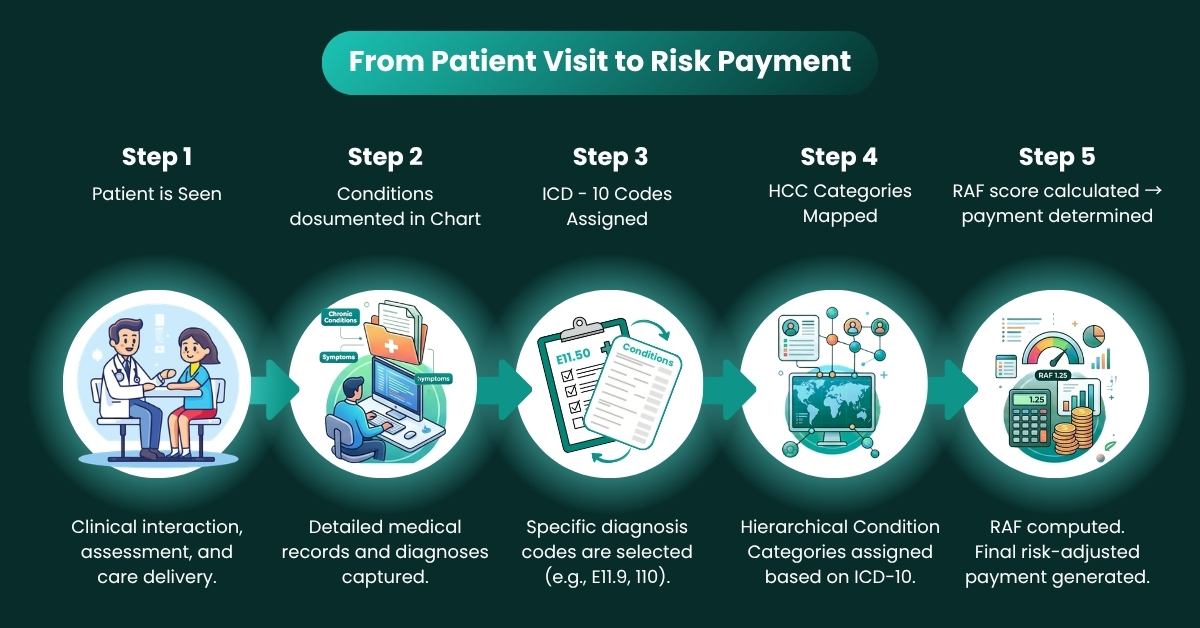
3. How the HCC Risk Adjustment Model Works
CMS-HCC model is based on a Risk Adjustment Factor (RAF) score that measures the cost that a patient is expected to incur compared to a typical Medicare patient. Any score of 1.0 is considered Average. If a patient has multiple chronic conditions, their RAF score would be greater than 1.0, and if a patient is relatively healthy, the score would be less than 1.0.
There are two key factors in the building of the RAF score:
- The demographics included age, gender, Medicaid dual eligibility and institutional status.
- Description of the disease or injury. From the previous year’s claim or encounter.Description of the disease or injury — ICD-10-CM codes from previous year’s claim / encounter.
The number assigned to each HCC category (a number that is added to the patient’s RAF score) is known as a coefficient. In some HCCs, there are also interactions between the other HCCs, which result in further score increments when certain combinations of conditions are met.
More detail on RAF score calculation is available through the CMS Advance Notice and Call Letter archives.
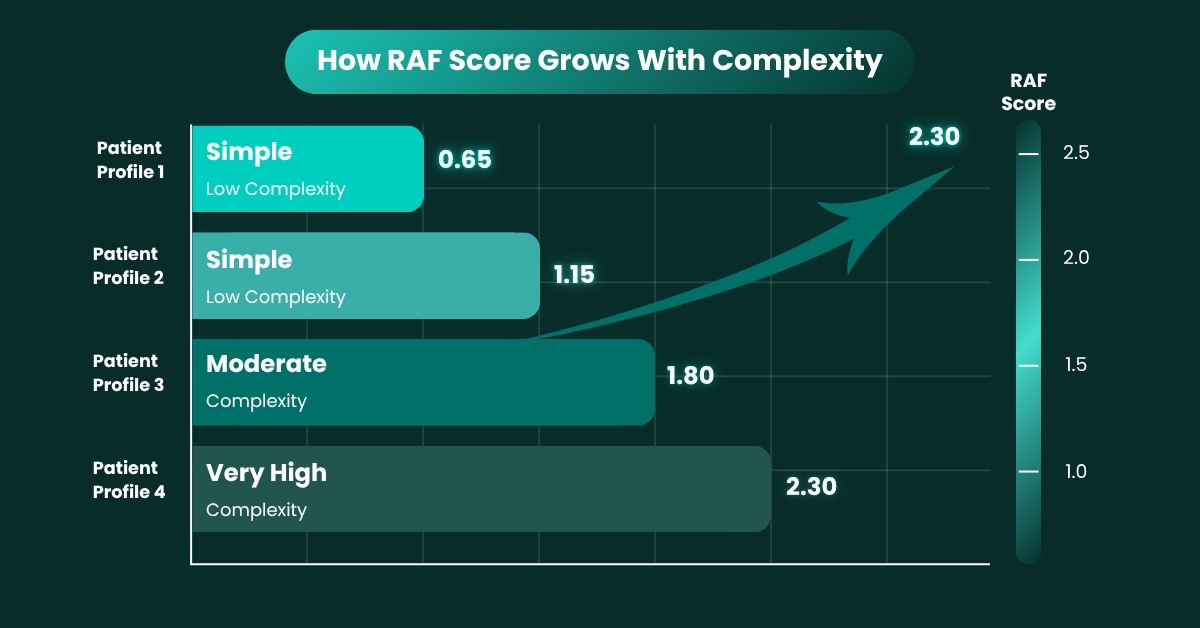
Risk Score by Patient Complexity — Reference Table
| Patient Profile | Documented HCC Conditions | Approximate RAF Score | Monthly Payment Impact |
|---|---|---|---|
| Low Complexity | None captured | 0.70 | Below baseline |
| Moderate Complexity | Diabetes + HTN | 1.25 | ~25% above baseline |
| High Complexity | CHF + CKD Stage 4 + Diabetes | 2.10 | ~110% above baseline |
| Very High Complexity | Cancer + CKD + Major Depression + PAD | 3.40+ | 240%+ above baseline |
Note: RAF scores shown are illustrative approximations. Actual scores vary based on CMS model year and patient-specific factors.
4. Common HCC Categories and Their ICD-10 Codes
All diagnoses are not considered HCCs. The following are the conditions that have been identified by CMS as ones that have a meaningful and predictable impact on healthcare costs and have been assigned to an HCC category. There is a reference table of the most common HCC categories used in clinical practice below.
| HCC Category | Example Conditions | ICD-10 Code Examples | Why It Matters |
|---|---|---|---|
| Cardiovascular Disease | Congestive Heart Failure, Chronic Ischemic Heart Disease | I50.9, I25.10 | High hospitalisation risk; significant cost weight |
| Diabetes with Complications | Diabetic Nephropathy, Diabetic Neuropathy | E11.65, E11.40 | Complications elevate RAF score considerably |
| Chronic Kidney Disease (CKD) | CKD Stage 3, CKD Stage 4 | N18.3, N18.4 | Stage-specific coding is required for accuracy |
| Respiratory Conditions | COPD, Chronic Respiratory Failure | J44.1, J96.10 | Impacts resource utilisation projections |
| Cancer & Tumors | Breast Cancer (active), Prostate Malignancy | C50.911, C61 | Active vs. history distinction is critical |
| Major Neurological Disorders | Hemiplegia, Multiple Sclerosis | G81.90, G35 | High functional impact; raises risk adjustment |
| Mental Health Conditions | Major Depressive Disorder, Schizophrenia | F33.1, F20.9 | Often underdocumented; affects overall RAF |
| Vascular Disease | Peripheral Artery Disease, Atherosclerosis | I73.9, I70.201 | Frequently missed; complicates care planning |
Source: CMS-HCC Model V28 (2024). ICD-10-CM codes are examples only; coding must reflect the documented specificity in each patient’s chart.
The word ‘hierarchical’ in HCC refers to the way similar conditions are ranked by severity. When a patient has both a less severe and a more severe version of the same condition for example, both Type 2 diabetes without complications and Type 2 diabetes with chronic kidney disease, only the highest-severity HCC in that group is counted. Duplicate coding does not inflate the score.
5. What Makes a Diagnosis Count for HCC?
Not all codes listed on a chart will go towards CMS risk adjustment. If you want to get a diagnosis to count:
- Must be documented by a qualified provider (MD, NP, PA, and other eligible clinicians)
- Must be documented in clinical detail; “possible” or “probable” are not acceptable terms.
- It must be discussed, evaluated or tracked during the encounter, a reference to it but not addressed, evaluated or monitored is not enough.
- It should be coded using the most specific ICD-10-CM code that can be used
- Must have a claim type that is eligible for risk adjustment (face-to-face services, not laboratory or ancillary services)
Specificity is everything in HCC coding. Documenting ‘diabetes’ is not the same as documenting ‘Type 2 diabetes with diabetic chronic kidney disease, stage 3.’ The latter maps to a higher-weighted HCC. Coders and providers should work together to ensure the level of specificity in the note matches what is coded.
6. Common HCC Coding Mistakes to Avoid
Even experienced practices run into documentation and coding gaps that affect HCC capture. These are the most frequently seen errors:
Underdocumentation of Chronic Conditions
A chronic condition that is known to exist but is not addressed in the note will not count. Physicians sometimes focus only on the presenting complaint and omit chronic conditions that are actively managed. A review of the problem list and medication list at each visit helps prevent this.
Coding to an Unspecified Level
ICD-10 codes like E11.9 (Type 2 diabetes mellitus without complications) carry less HCC weight than more specific codes that reflect existing complications. When documentation supports a more specific diagnosis, the more specific code should always be used.
Annual Recapture Gaps
Because the CMS-HCC model requires annual recapture, a chronic condition that was coded last year but not this year will drop out of the risk score. Practices without a systematic annual recapture process often see unexplained decreases in RAF scores.
Missing Condition Interactions
Certain HCC combinations carry interaction coefficients that increase the RAF score beyond the sum of the individual HCCs. For example, the interaction between diabetes and congestive heart failure is weighted additionally. Coders who are not aware of these interactions miss part of the score.
Relying on Coders Without Clinical Validation
HCC coding is not a purely administrative function. It requires clinical context. Coders reviewing charts must have access to the full clinical picture, and providers must be available for queries when documentation is ambiguous.
7. HCC Coding in the Context of Value-Based Care
The shift from volume-based to value-based care has made HCC coding more relevant than ever. Under programs such as the Medicare Shared Savings Program (MSSP) and Medicare Advantage, provider payment is increasingly tied to patient outcomes, quality metrics, and cost efficiency.
Accurate HCC coding contributes to this in two important ways. First, it ensures that the risk-adjusted benchmarks used to evaluate a practice’s performance actually reflect the complexity of the patient population being served. A practice with a sicker-than-average panel should not be measured against benchmarks built for healthier populations. Second, it enables better care coordination because the conditions that drive cost the chronic, complex ones, are formally on record and can be tracked.
The CMS Innovation Center provides ongoing resources on value-based models and how risk adjustment plays a role in each.
8. How HCC Audits Work
CMS conducts Risk Adjustment Data Validation (RADV) audits to verify that the diagnoses submitted for risk adjustment are supported by the medical record. During a RADV audit, a sample of enrollees is reviewed, and for each enrollee, specific HCC diagnoses must be confirmed in the documentation.
If a submitted HCC cannot be validated in the record, a payment error rate is calculated, and extrapolated recoupment may follow. This is why documentation quality matters as much as the coding itself.
- The medical record must contain the diagnosis, not just a code on a claim
- The documentation must be dated within the applicable data collection period
- The provider must be a credentialed, eligible clinician
- The note must support the specificity of the code submitted
More on RADV methodology can be reviewed through CMS’s RADV resources.
CMS has moved to implement extrapolation in RADV audits, meaning a payment error found in a sample can be projected across all claims for an audit period. A small percentage of underdocumented codes can result in a large recoupment demand. Proactive internal auditing is significantly less costly than reactive repayment
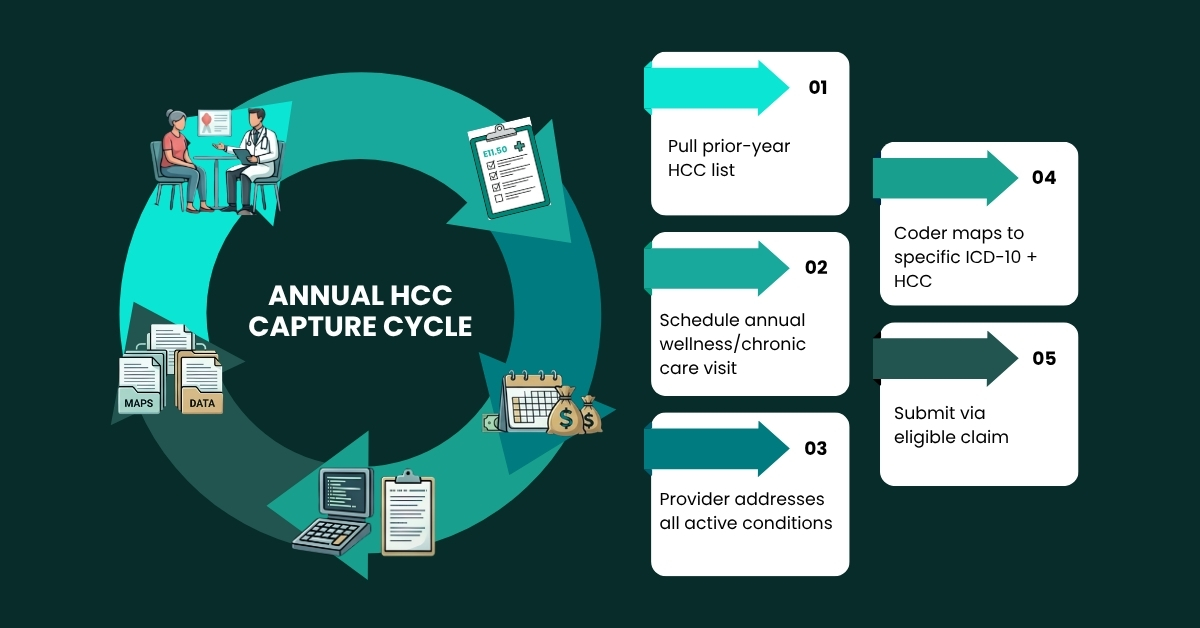
9. Best Practices for Improving HCC Capture
Sustainable improvement in HCC coding capture comes from building the right habits across the clinical and administrative team, not just from periodic coding reviews.
Conduct Annual HCC Reviews
At the start of each calendar year, a review of each patient’s prior-year HCC diagnoses should be initiated. Any chronic condition that was coded previously and is still active needs to be addressed and recoded in a current encounter.
Integrate HCC Prompts Into the EHR Workflow
Many EHR platforms support HCC risk-capture alerts that flag when a patient has a known chronic condition not yet documented in the current year. These prompts reduce the risk of annual recapture gaps.
Train Providers on Documentation Specificity
Brief, periodic education sessions for clinical staff on the link between note specificity and coding outcomes go a long way. Providers do not need to know every HCC code number — but they do need to understand that the way they phrase a diagnosis in the note has downstream financial and clinical consequences.
Establish a Coder-Provider Query Process
When a coder identifies a potential HCC diagnosis in the chart but documentation is insufficient to support the code, a formal query process should be in place for the provider to clarify. Unresolved queries are missed revenue.
Perform Prospective HCC Gap Analysis
Rather than coding only what appears in today’s note, a prospective gap analysis compares the current year’s coded HCCs against the prior year’s submitted conditions. Any condition that is missing from the current year represents a coding gap to be investigated.
Final Thoughts
HCC coding is not a compliance formality. It is the mechanism through which the complexity of a patient population is formally recognized in the payment system. When it is done well, providers are compensated appropriately, care plans are better informed, and audit risk is minimized.
The practices that invest in accurate, complete HCC documentation do not just protect revenue, they build a more accurate picture of the patients they serve, which ultimately supports better clinical decision-making.
- Missed HCC codes mean lost revenue and inaccurate risk scores. Vigilant Medical Billing Group specializes in thorough, compliant HCC coding reviews that protect your bottom line and your patients’ care.