Introduction To Medical Coding and Billing Abbreviations:
Medical coding and billing don’t run on full sentences, they go on abbreviations. Like from CPT and ICD-10, to EOB, ERA, and CARC codes, every step of the revenue cycle depends on shorthand that affects how fast and how accurately providers get paid. The problem is, most errors, denials and delays don’t show up because the case is overly complex, but because some acronym was misused or misunderstood.
The CMS data shows that claim denials cost the U.S. healthcare system billions of dollars each year because medical coding and billing errors which stem from misunderstood abbreviations make up a large portion of the denials.
This blog provides one trustworthy medical coding abbreviations list which includes medical billing abbreviations to create a common vocabulary for all healthcare practice employees, front-desk staff, certified coders, practice managers, and physicians, establishing a shared language which prevents errors and decreases denial rates while also speeding up the reimbursement processes.
The Complete Medical Coding Abbreviations List
Medical coding involves translating clinical services, diagnoses, and procedures into standardized codes. The following medical coding abbreviations are the most widely used across practices in the United States.
| Abbreviation | Full Form | Definition / Usage |
|---|---|---|
| CPT | Current Procedural Terminology | The AMA-maintained code set used to report medical procedures and services. |
| ICD-10-CM | International Classification of Diseases, 10th Revision, Clinical Modification | Diagnosis coding system required for all U.S. healthcare claims since 2015. |
| ICD-10-PCS | ICD-10 Procedure Coding System | Used by hospitals for inpatient procedure coding. |
| HCPCS | Healthcare Common Procedure Coding System | Extends CPT codes; includes Level I (CPT) and Level II (non-physician services, DME, drugs). |
| DRG | Diagnosis-Related Group | A classification system used for hospital inpatient reimbursement under Medicare. |
| E&M | Evaluation and Management | CPT codes (99202–99499) for office visits and clinical decision-making encounters. |
| MUE | Medically Unlikely Edit | CMS-established maximum units of service allowed per claim line. |
| CCI | Correct Coding Initiative | Edits by CMS that prevent improper payment of CPT code combinations. |
| NCCI | National Correct Coding Initiative | The national version of CCI used by Medicare to detect coding errors. |
| PCS | Procedure Coding System | Short reference to ICD-10-PCS in inpatient hospital settings. |
| NEC | Not Elsewhere Classified | Used in ICD-10 when no specific code is available for a condition. |
| NOS | Not Otherwise Specified | A catch-all code when no further specificity is documented. |
| CC | Complication/Comorbidity | An additional diagnosis that affects DRG assignment and reimbursement. |
| MCC | Major Complication/Comorbidity | A condition that significantly increases the complexity of inpatient care. |
| PDX | Principal Diagnosis | The condition chiefly responsible for a hospital admission. |
| SOI | Severity of Illness | A measure used in APR-DRG systems to categorize patient complexity. |
| ROM | Risk of Mortality | Used alongside SOI to reflect the likelihood of death in inpatient care. |
| APC | Ambulatory Payment Classification | The outpatient equivalent of DRGs used by CMS for hospital reimbursements. |
| ASC | Ambulatory Surgical Center | A facility type affecting coding, place of service codes, and reimbursement rates. |
| POS | Place of Service | A two-digit code on claims indicating where the service was delivered. |
This medical coding abbreviations list represents the important terms encountered in daily coding work. Specialty coders who work in anesthesia and cardiology and orthopedics will use additional specialized codes and modifiers which exist outside the standard code list.
The shift from ICD-9 to ICD-10-CM in October 2015 increased the number of diagnosis codes from approximately 14,000 to over 70,000. Many practices that lacked proper training in the new coding abbreviations and specificity requirements saw claim denial rates spike significantly in the months following the transition.
Medical Billing Abbreviations List You Must Know
| Abbreviation | Full Form | Definition / Usage |
|---|---|---|
| EOB | Explanation of Benefits | A document from a payer explaining how a claim was processed, including amounts paid, adjusted, and patient responsibility. |
| ERA | Electronic Remittance Advice | The electronic version of the EOB, transmitted via EDI 835 transaction sets. |
| EFT | Electronic Funds Transfer | Direct deposit of insurance reimbursements into a provider's bank account. |
| EDI | Electronic Data Interchange | The electronic exchange of healthcare claim data between providers and payers. |
| NPI | National Provider Identifier | A unique 10-digit identifier assigned to every healthcare provider by CMS. |
| TIN | Tax Identification Number | Required on all claims for group practices and billing entities. |
| EIN | Employer Identification Number | A federal tax ID used by group practices to identify their billing entity. |
| A/R | Accounts Receivable | Outstanding claim balances owed to the provider by payers or patients. |
| AR | Accounts Receivable | See A/R; used interchangeably in billing workflows. |
| UB-04 | Uniform Billing 04 | The standardized claim form used by hospitals and facilities for inpatient and outpatient billing. |
| CMS-1500 | Centers for Medicare & Medicaid Services (1500 Form) | The standard claim form used by physicians and non-facility providers. |
| PA | Prior Authorization | Advance approval from a payer required before certain services can be rendered. |
| RA | Remittance Advice | The document that accompanies payment, explaining claim adjustments and denials. |
| CO | Contractual Obligation | A claim adjustment reason code indicating a write-off per provider-payer contract. |
| PR | Patient Responsibility | The portion of a claim balance owed by the patient after payer adjudication. |
| OA | Other Adjustment | A payer adjustment that does not fall under CO or PR categories. |
| CARC | Claim Adjustment Reason Code | Codes used by payers to explain claim adjustments on remittance advice. |
| RARC | Remittance Advice Remark Code | Supplemental codes providing additional context alongside CARCs. |
| ANSI | American National Standards Institute | The standards body that defines EDI transaction formats, including 837P and 837I. |
| 837P | ANSI 837 Professional | The electronic claim format used by physicians and non-institutional providers. |
| 837I | ANSI 837 Institutional | The electronic claim format used by hospitals and facility providers. |
| 277CA | Claim Acknowledgment | An electronic transaction from a payer acknowledging receipt of a claim batch. |
| 270/271 | Eligibility Inquiry / Response | EDI transactions used to verify patient insurance eligibility before service. |
| COB | Coordination of Benefits | The process of determining which payer is primary when a patient has multiple insurances. |
| PAR | Participating Provider | A provider who has signed a contract with a payer and accepts negotiated rates. |
| NON-PAR | Non-Participating Provider | A provider with no contract with a given payer; may balance bill patients. |
| OON | Out-of-Network | Services provided by a non-contracted provider, usually resulting in higher patient cost-sharing. |
| HIPAA | Health Insurance Portability and Accountability Act | Federal law governing patient data privacy, electronic transactions, and security. |
| PHI | Protected Health Information | Any individually identifiable health information governed by HIPAA. |
| RCM | Revenue Cycle Management | The full financial process from patient scheduling through final payment collection. |
Learn about VMG’s Denial Management Services to reduce claim rejections with expert support at every step.
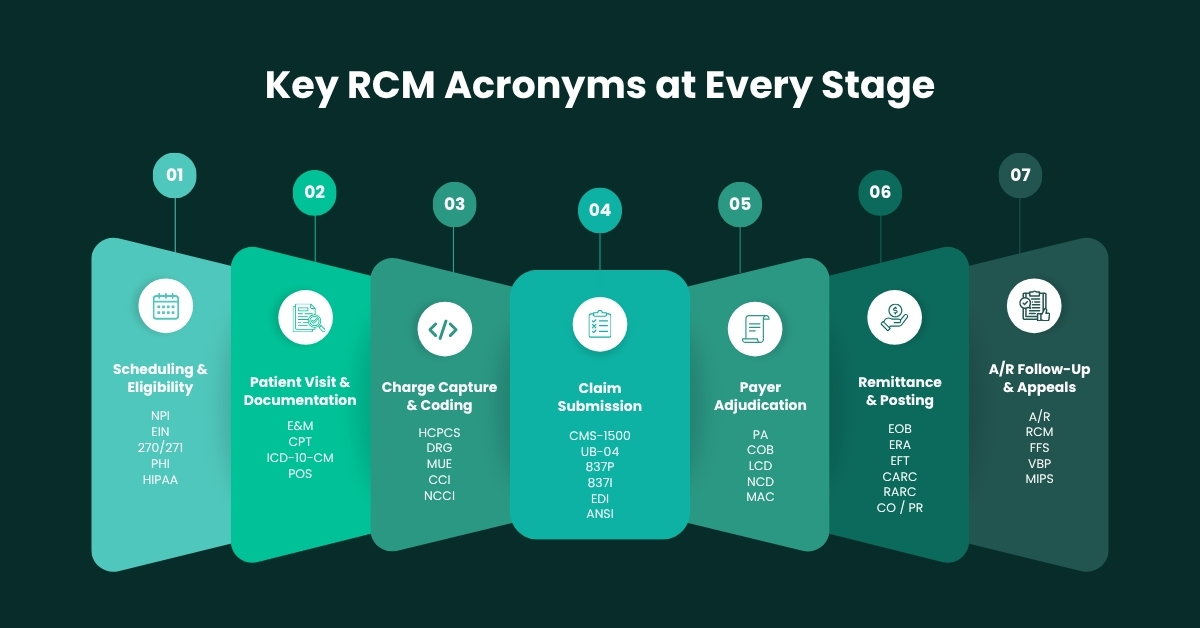
Essential Healthcare Acronyms for Revenue Cycle Management
| Acronym | Full Form | Definition / Usage |
|---|---|---|
| CMS | Centers for Medicare & Medicaid Services | The federal agency overseeing Medicare, Medicaid, CHIP, and ACA marketplace plans. |
| AMA | American Medical Association | The organization that maintains CPT codes and physician professional standards. |
| AAPC | American Academy of Professional Coders | A major certification body for medical coders (CPC, CRC, COC credentials). |
| AHIMA | American Health Information Management Association | A professional organization for health information and coding professionals (CCS, RHIA credentials). |
| CPC | Certified Professional Coder | An AAPC credential for outpatient coding specialists. |
| CCS | Certified Coding Specialist | An AHIMA credential for coding specialists, particularly in hospital settings. |
| MAC | Medicare Administrative Contractor | A private company contracted by CMS to process Medicare claims in a specific jurisdiction. |
| LCD | Local Coverage Determination | A MAC's policy defining when a specific service is covered under Medicare locally. |
| NCD | National Coverage Determination | A CMS policy defining Medicare coverage of a service nationwide. |
| FQHC | Federally Qualified Health Center | A community health center receiving federal funding with special billing rules. |
| FFS | Fee-for-Service | A payment model where providers are reimbursed per individual service rendered. |
| VBP | Value-Based Purchasing | A CMS payment model that ties reimbursement to quality and outcome metrics. |
| ACO | Accountable Care Organization | A group of providers coordinating care for a shared patient population under CMS programs. |
| MIPS | Merit-based Incentive Payment System | A CMS value-based payment track under MACRA affecting physician reimbursements. |
| MACRA | Medicare Access and CHIP Reauthorization Act | A 2015 law restructuring Medicare physician payment into quality-based tracks. |
| DME | Durable Medical Equipment | Medical equipment for home use (e.g., wheelchairs, CPAP machines) billed under HCPCS Level II. |
| DMEPOS | Durable Medical Equipment, Prosthetics, Orthotics, and Supplies | Broader category encompassing DME plus related items billed to Medicare/Medicaid. |
| SNF | Skilled Nursing Facility | A facility providing post-acute care with specific billing rules under Medicare Part A. |
| HHA | Home Health Agency | A provider of in-home healthcare services billed under Medicare Home Health benefit. |
| ASA | American Society of Anesthesiologists | The professional body that maintains the ASA Physical Status Classification and anesthesia billing guidelines. |
Medical Coding vs. Medical Billing Abbreviations
The blurring of coding and billing functions creates common confusion problems which occur in healthcare practices. The comparison table below shows the main focus area of each function together with its important abbreviations and associated governing bodies and operational tools.
| Category | Medical Coding | Medical Billing |
|---|---|---|
| Primary Role | Translate clinical documentation into standardized codes | Submit codes to payers and manage payment collection |
| Key Abbreviations | CPT, ICD-10-CM, HCPCS, DRG, E&M, MUE, CCI, POS, APC, NEC | EOB, ERA, EDI, NPI, A/R, CMS-1500, UB-04, PA, CARC, RARC |
| Healthcare Acronyms | AMA, AAPC, AHIMA, CPC, CCS, LCD, NCD | CMS, HIPAA, MAC, RCM, COB, ANSI, EFT |
| Governing Standards | CPT manual (AMA), ICD-10 (WHO/CMS), HCPCS (CMS) | HIPAA transactions, CMS-1500/UB-04 guidelines |
| Certification Bodies | AAPC (CPC, CRC), AHIMA (CCS, RHIA) | AAPC (CPB), HFMA, MGMA |
| Error Impact | Wrong code = wrong payment or denial at submission | Wrong form/EDI = rejection before adjudication |
| Tools Used | EHR coding modules, encoder software, NCCI edits | Practice management systems, clearinghouses, payer portals |
| Claim Stage | Pre-submission (charge capture) | Post-coding (claim submission to payment posting) |
| Connection to Revenue | Determines reimbursement level | Ensures that determined amount is actually collected |
According to the American Medical Association, nearly 1 in 7 medical claims submitted to Medicare is denied on first submission. The majority of these denials result from incorrect or incomplete coding which includes wrong ICD-10-CM diagnosis codes and misused CPT modifiers and place of service errors. For practices that are not fluent in the medical coding abbreviations list, every submission carries unnecessary financial risk.
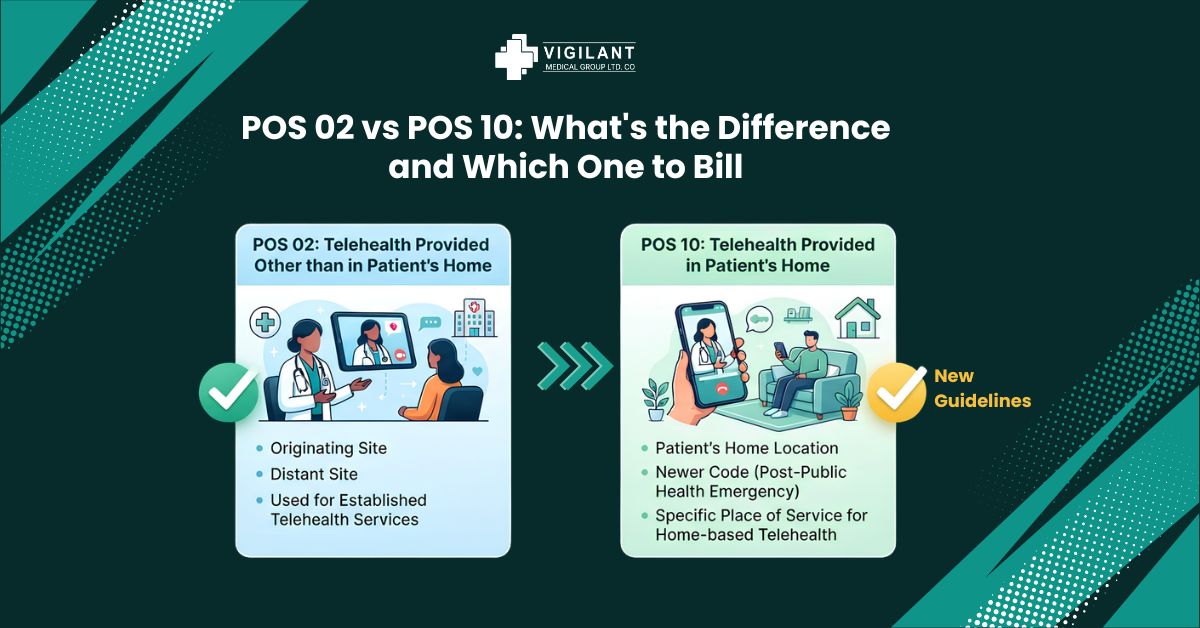
The incorrect usage of Place of Service (POS) codes stands as the foremost cause that leads to claim denials, but which medical practitioners can easily avoid. The procedure which occurs at an Ambulatory Surgical Center (ASC) requires proper coding with POS 24 while the same procedure needs its office-based implementation to use POS 11. The reimbursement rates differ because CMS establishes separate payment rates for facility services and non-facility services. The actual site of service must serve as the basis for confirming POS codes instead of using only the provider’s primary practice address. The process of handling EOBs and ERAs becomes difficult when people mistakenly think CARCs (Claim Adjustment Reason Codes) are the same thing as RARCs (Remittance Advice Remark Codes). CARCs provide reasons which explain payment reductions and payment denials while RARCs present additional information. The complete picture of required corrective actions emerges from reading both documents together instead of reading them separately. The American Society of Anesthesiologists (ASA) units used in anesthesia practices differ from standard CPT time units in their calculation method. Anesthesia practitioners often under bill their services because they do not understand how to use base units together with time units.
Explore VMG’s Anesthesia Medical Coding Services for specialty specific coding expertise.
Most Frequently Searched Medical Billing Acronyms
The following graph represents approximate relative search frequency for key medical billing acronyms among healthcare professionals based on industry keyword data from 2024–2025. These terms consistently appear in the most common billing training materials, payer guidelines, and denial management workflows.
Frequently Asked Questions (FAQs)
Q1: What is the difference between CPT and HCPCS codes?
CPT codes, which the American Medical Association maintains, serve to identify physician services plus outpatient medical procedures. HCPCS, which the Healthcare Common Procedure Coding System uses, contains both Level I CPT codes and Level II codes that describe non-physician medical practices including ambulance services and durable medical equipment and injectable drugs. Organizations use both systems to process claims but each system serves distinct functions for medical billing.
Q2: What does EOB stand for in medical billing?
The term EOB is an abbreviation that stands for Explanation of Benefits in the context of medical billing. The payer (insurance company) issues the document after a claim gets processed to show the details of payment which includes the paid amount plus adjusted values and the remaining patient debt. The document functions separately from the Electronic Remittance Advice (ERA) which serves as the digital equivalent used in practice management systems.
Q3: What is RCM in healthcare?
RCM stands for Revenue Cycle Management. Healthcare organizations use RCM to manage their revenue cycles. The financial operations of a healthcare practice, which track patient care from registration through to final payment, constitute the complete financial workflow of revenue cycle management. The revenue cycle management process includes six steps, which are coding, billing, claims submission, denial management, A/R follow-up, and patient collections.
Q4: Why is NPI important in medical billing?
The National Provider Identifier functions as a unique identification number, which CMS assigns to every healthcare provider with a 10-digit number. Every claim submission requires the NPI number for both CMS-1500 and UB-04 forms. A missing, incorrect, or expired NPI is one of the top reasons claims are rejected before even reaching adjudication.
Q5: What are CARC and RARC codes?
CARC stands for Claim Adjustment Reason Code, and RARC stands for Remittance Advice Remark Code. CARCs explain why a claim payment was reduced or denied (e.g., CO-45 for contractual adjustment, PR-1 for deductible). RARCs provide supplementary information to clarify the CARC. Both appear on EOBs and ERAs and are essential reading for any billing team managing denials and follow-ups.
Q6: Is ICD-10-CM the same as ICD-10-PCS?
No. ICD-10-CM (Clinical Modification) is used for diagnosis coding across all care settings in the United States. ICD-10-PCS (Procedure Coding System) is used exclusively for inpatient hospital procedure coding. Outpatient and physician procedures are coded using CPT codes, not
Final Thoughts
The language of healthcare billing is dense, specialized, and constantly evolving. The medical coding and billing abbreviations and the healthcare acronyms used in RCM represent the essential vocabulary needed for revenue cycle operations. Organizations that establish training programs for their employees to learn these abbreviations and who collaborate with specialized billing firms that fully understand this terminology achieve superior results compared to organizations that regard billing as not an essential task. Organizations spending time on employee training achieves improved financial results through its operational processes which results in reduced denial rates and quicker payment times as well as increased compliance and enhanced revenue streams. New codes are added to CPT and ICD-10-CM every year. CMS updates LCD and NCD policies regularly. Payers introduce new CARC and RARC codes. HIPAA transaction standards get revised. In this environment, a static knowledge of medical coding abbreviations and medical billing abbreviations is not enough, it needs to be maintained and applied every day.
Partnering with expert billing companies who live and breathe this language consistently outperform those that treat billing as an afterthought. Fewer denials, faster reimbursements, better compliance, and stronger cash flow are not accidents. They are the results of doing billing the right way.
At Vigilant Medical Group, our AAPC-certified coders and billing specialists handle every abbreviation, every modifier, every place of service code, and every claim adjustment with precision. From anesthesia RCM to general medical billing across all specialties, we bring expertise that translates directly into revenue for your practice.