“Provider credentialing is an essential process which is vital for healthcare providers to bill insurance and get reimbursements. This is the formal process by which insurance companies verify whether a hospital and healthcare organizations meet specific standards in terms of education, training, licensing and competency.”
Delay is usually caused by factors like an application that is incomplete, or trouble tied to a malpractice history, which makes it take longer than expected.
This blog explains what provider credentialing is, who needs to be credentialed, what the whole checklist looks like, and the usual timeline, which can run 90–120 days. Complexities of telehealth credentialing is also discussed and a checklist template you can use to streamline your credentialing efforts.
Overall, good credentialing management is crucial for keeping revenue steady in healthcare practices.
What Is Provider Credentialing?
Provider credentialing is the formal process by which insurance companies, hospitals, and healthcare organizations verify that a physician or other healthcare provider meets specific standards of education, training, licensure, and competency. Without it, you literally cannot bill insurance.
No credentialing = no reimbursements.
But here’s what most people don’t realize: credentialing isn’t just a formality. It’s a gatekeeping process that insurers take very seriously. Payers want to know that every provider in their network is qualified, licensed, and has a clean professional record. Any red flag and they’ll hold your application indefinitely.
Industry data suggests that credentialing delays account for revenue losses ranging from $10,000 to over $30,000 per month for a single provider. For group practices, that number multiplies fast.
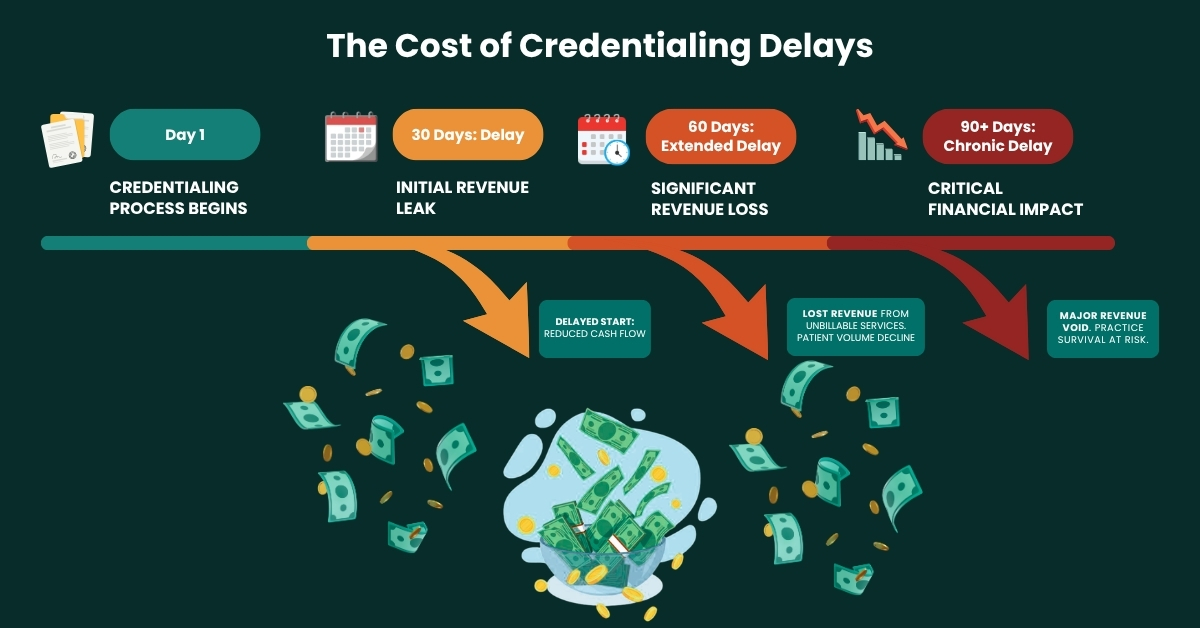
According to the Council for Affordable Quality Healthcare (CAQH), the average credentialing cycle takes 90–120 days. That’s three to four months where you’re seeing patients but potentially billing nothing or worse, billing incorrectly and getting retroactive claim denials.
For a complete breakdown of how the credentialing process works with Medicare, visit the CMS Provider Enrollment Resource. It’s one of the most authoritative external references available.
Who Needs to Be Credentialed?
A common question we get at Vigilant Medical Group is: does every provider need to go through this? The answer is yes but the specifics vary.
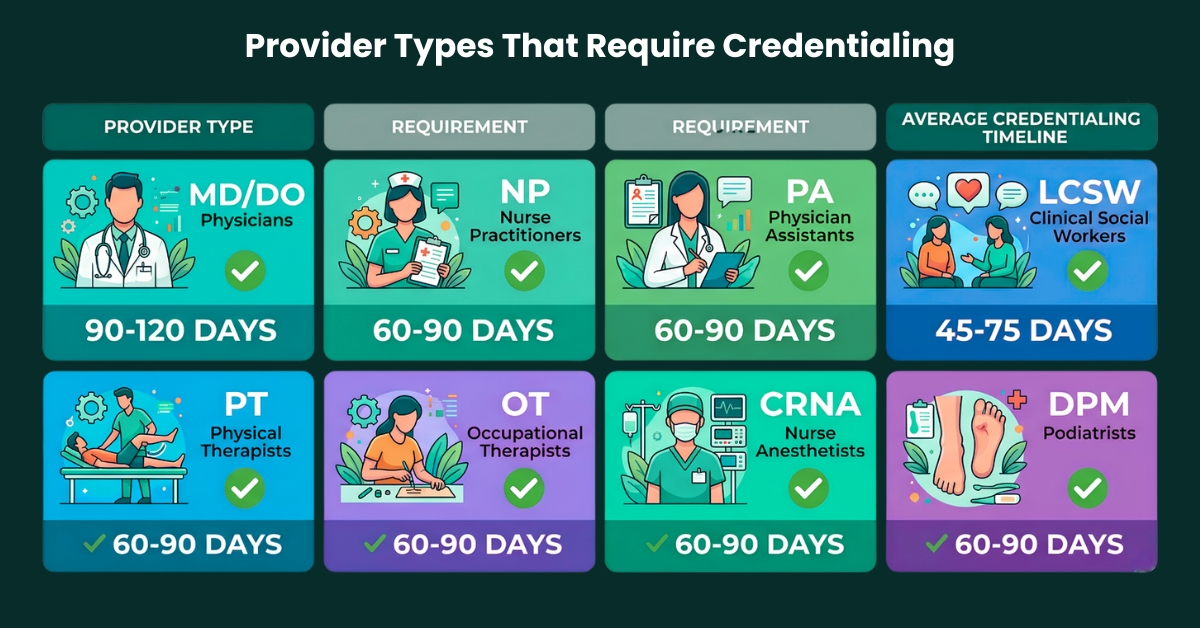
The following healthcare professionals typically need to complete the full physician credentialing checklist:
- Medical Doctors (MDs) and Doctors of Osteopathic Medicine (DOs)
- Nurse Practitioners (NPs) and Physician Assistants (PAs)
- Dentists and dental specialists
- Mental health providers; Psychologists, LCSWs, LPCs
- Physical, Occupational, and Speech Therapists
- Chiropractors and podiatrists
- Certified Nurse Midwives and CRNAs
Each payer (Aetna, BlueCross, United Healthcare, Medicaid, Medicare, etc.) has its own credentialing requirements and timelines which is precisely why having a universal provider credentialing checklist template is so valuable. You build it once, adapt it per payer, and stop scrambling every time you add a new insurance contract.
The Complete Provider Credentialing Checklist:
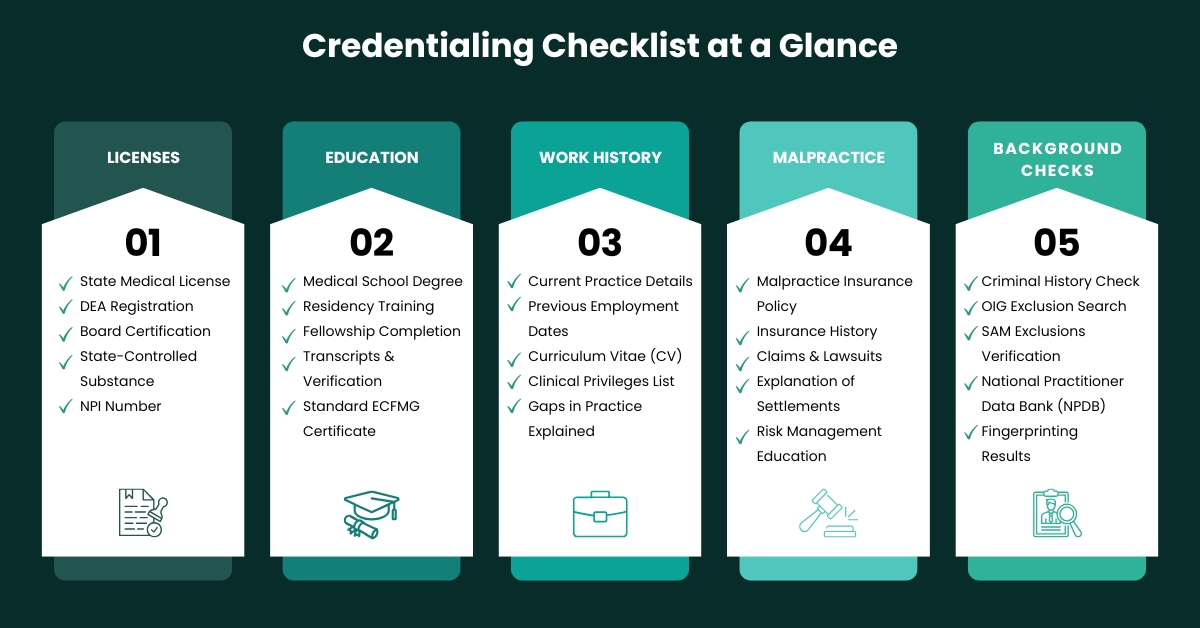
Below is the most comprehensive credentialing checklist for physicians and allied health providers currently in use. We’ve organized it into the key categories that every major payer will request.
| Category | Required Document | Status |
|---|---|---|
| License & Certifications | State medical license (active) | ✅ / ❌ |
| License & Certifications | DEA registration (if applicable) | ✅ / ❌ |
| License & Certifications | Board certification documents | ✅ / ❌ |
| License & Certifications | NPI (Type 1 & 2) | ✅ / ❌ |
| Education & Training | Medical school diploma | ✅ / ❌ |
| Education & Training | Residency completion certificate | ✅ / ❌ |
| Education & Training | Fellowship certificate (if any) | ✅ / ❌ |
| Work History | Last 10 years employment history | ✅ / ❌ |
| Work History | Gap explanations (>30 days) | ✅ / ❌ |
| Malpractice | Current malpractice insurance certificate | ✅ / ❌ |
| Malpractice | Claims history (5–10 years) | ✅ / ❌ |
| Background Check | Criminal background check | ✅ / ❌ |
| Background Check | OIG/SAM exclusion check | ✅ / ❌ |
| Privileges | Hospital privilege letters (if applicable) | ✅ / ❌ |
| References | 3 peer references with contact info | ✅ / ❌ |
A. Licenses & Certifications
Your active state medical license is the foundation of everything. Make sure it’s:
- Current, not expired
- Not on probation
- Not under investigation.
Payers do real-time verification through sources like the National Practitioner Data Bank (NPDB) and state medical board websites. Your NPI (National Provider Identifier) Type 1 (individual) and Type 2 (organizational) both must be active in the NPPES database.
B. Education & Training
Every degree matters. Payers want verified transcripts or diplomas from accredited institutions not copies you print from your files, but verification through primary sources. This means your medical school and residency program may receive direct outreach from the payer’s credentialing team.
If you completed a fellowship or any specialty training, include all documentation. Unexplained gaps in your training history are a red flag that will trigger additional review.
C. Work History (Last 10 Years)
One of the most overlooked sections of any credentialing checklist template is employment history. Payers typically require a full 10-year work history, with explanations for any gaps exceeding 30 days. Yes, 30 days. So if you took three months off between jobs, you need a written explanation on file.
This is where many applications get stuck. Providers forget to account for locum tenens positions, sabbaticals, or periods of private practice. Be exhaustive and accurate here.
D. Malpractice Insurance & Claims History
You must provide a current Certificate of Insurance (COI) from your malpractice carrier. Most payers require minimum coverage of $1M per occurrence / $3M aggregate, though this varies by specialty and state.
Your malpractice claims history (typically 5–10 years) is one of the most scrutinized parts of the file. If you have prior claims, closed cases, or settlements, you’ll need to provide detailed explanations. Having documentation prepared in advance dramatically speeds this up.
E. Background Check & Exclusion Verification
Federal payers (Medicare, Medicaid) require that providers are NOT excluded from participation. Check the OIG List of Excluded Individuals and Entities (LEIE) and the SAM.gov database. If a provider is excluded and still billing federal programs, you’re looking at significant legal liability.
Many private payers now also run criminal background checks as part of their credentialing checklist for physicians.
The Credentialing Timeline
| Timeline | Stage | What Happens |
|---|---|---|
| Week 1 | Application Submission | Submit CAQH profile + payer-specific application |
| Week 2–3 | Primary Source Verification | Licenses, education, malpractice verified by payer |
| Week 4–6 | Committee Review | Credentialing committee evaluates provider file |
| Week 7–8 | Approval / Re-query | Payer grants approval or requests missing docs |
| Week 9–12 | Effective Date Issued | Provider is enrolled and can begin billing |
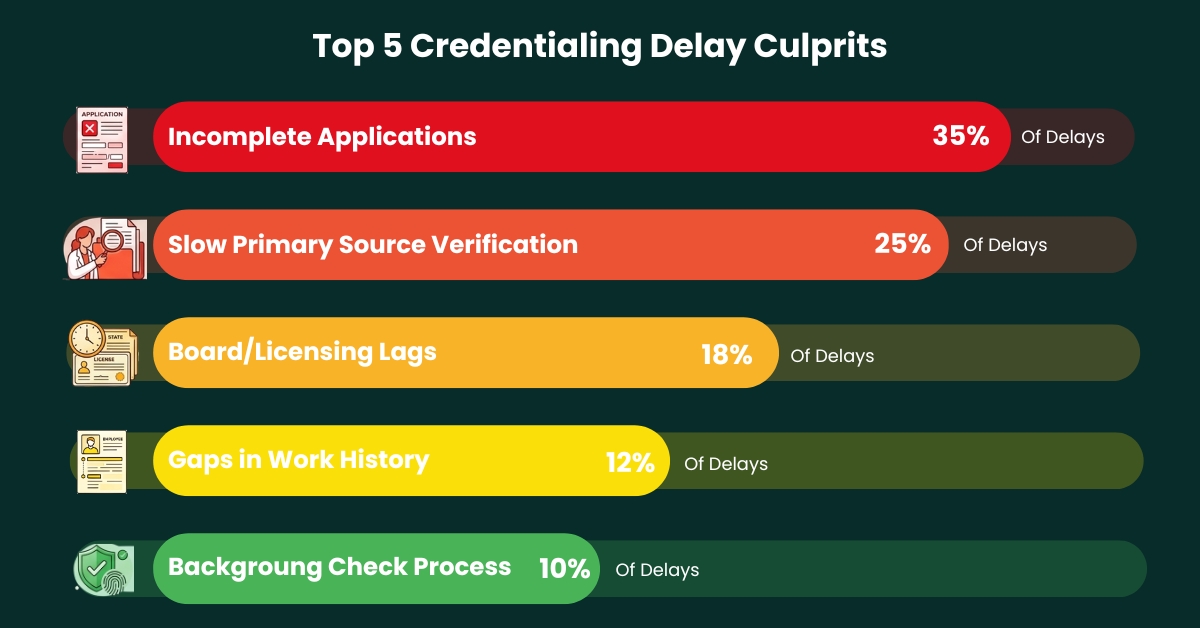
Why Applications Get Delayed
| Reason | Frequency |
|---|---|
| Incomplete Applications | ████████████████████ 42% |
| Malpractice History Issues | ████████████ 25% |
| License Verification Delays | █████████ 18% |
| Missing Work History Gaps | ██████ 12% |
| Reference Delays | █ 3% |
CAQH: Council for Affordable Quality Healthcare
If you haven’t heard of CAQH ProView, you need to know about it right now. CAQH (Council for Affordable Quality Healthcare) is a centralized credentialing database used by over 900 participating health plans. Instead of filling out a separate application for every payer, you complete one CAQH profile and payers pull from it directly.
Here’s what makes CAQH critical to your credentialing checklist:
- Your CAQH profile must be 100% complete, missing fields will cause payer rejections
- You must re-attest your profile every 120 days, or it expires and delays your credentialing
- All documents in CAQH must be current, outdated references are flagged instantly
- CAQH is free for providers but requires consistent maintenance
Providers can register and manage their profile directly at proview.caqh.org. If you’re a group practice managing multiple provider profiles, this becomes a full-time job which is why practices outsource credentialing management to specialists.
Group Practice Credentialing vs. Individual Provider Credentialing
There’s an important distinction between credentialing an individual provider and credentialing within a group practice. Many providers assume that once the practice is credentialed, they’re automatically covered. That’s not always true.
In group practice credentialing, each individual provider still needs to be credentialed with each payer. What changes is that the group’s Tax ID and organizational credentials are also verified. This means double the documentation in some cases.
For group practices, the provider credentialing checklist must also include:
- IRS EIN (Employer Identification Number) with tax documentation
- Group NPI (Type 2) separate from individual NPIs
- Business license and accreditation certificates
- Group malpractice policy in addition to individual coverage
- Practice location addresses verified with each payer
Maintaining Credentials: The Ongoing Responsibility
Credentialing doesn’t end when you get your approval letter. Re-credentialing is a reality every provider faces. Most payers require re-credentialing every 2–3 years. Hospitals often require it annually. Miss a re-credentialing cycle, and you can be removed from a payer network which means claim denials going back to the gap period.
Your ongoing credentialing maintenance checklist should include:
- Track license renewal dates
- Keep CAQH updated with every job change, address change, and policy renewal
- Monitor malpractice policy expiration and renew before it lapses
- Watch for state medical board notifications and NPDB self-queries annually
- Keep continuing education (CME) records updated Verify DEA registration renewal (DEA registrations expire every 3 years)
This is where having a dedicated credentialing partner makes an enormous difference. A credentialing specialist proactively tracks all expiration dates and initiates renewals on your behalf.
Credentialing Red Flags That Trigger Automatic Delays And How to Avoid Them
Payer credentialing committees are not particularly forgiving. Certain red flags almost always result in an extended review or outright deferral:
Unexplained Employment Gaps: Any gap over 30 days without a written explanation attached will trigger additional committee review. Always include a brief, professional letter explaining the gap.
Malpractice Claims Without Context: A malpractice claim doesn’t automatically disqualify you. But a malpractice claim with no attached explanation, case outcome, or settlement documentation almost always causes delays.
License Encumbrances: Probation, suspension, or any disciplinary action from a state medical board must be disclosed. Payers check the NPDB. If you don’t disclose it and they find it, your application is typically rejected entirely.
Incomplete References: Three peer references are standard. If even one doesn’t respond within the credentialing window, the application stalls. Choose references who are responsive and who know you professionally.
Address Mismatches: Your practice address must match exactly across your NPI record, CAQH profile, and payer application. Even a street abbreviation mismatch “St” vs. “Street” can cause system-level rejection.
Should You Handle Credentialing In-House or Outsource It?
| Factor | In-House Credentialing | Outsourced Credentialing |
|---|---|---|
| Cost | Staff salary + training + software | Fixed monthly fee |
| Speed | Slower, the staff handles multiple tasks | Dedicated specialists = faster turnaround |
| Expertise | Requires ongoing training | Deep, specialized knowledge |
| Errors | Higher risk if staff is overwhelmed | Systematic processes reduce errors |
| Scalability | Hard to scale with practice growth | Easily handles multiple providers |
| Follow-up | Often missed or inconsistent | Proactive weekly payer follow-up |
Telehealth Credentialing
If you offer telehealth services, credentialing requirements become even more complex. Many payers require separate credentialing or enrollment for telehealth services, and several states have unique telehealth-specific licensure requirements.
Your telehealth credentialing checklist additions:
- State telehealth licensure for each state where patients are located (not just where you’re based)
- Telehealth-specific modifiers and place-of-service codes aligned with payer policies
- HIPAA-compliant technology platform documentation (some payers require this)
- Telehealth credentialing with CMS if billing Medicare/Medicaid telehealth
The American Telemedicine Association (ATA) offers updated guidance at americantelemed.org a useful external resource for providers navigating multi-state telehealth credentialing.
Your Free Credentialing Checklist Template: Download & Use Today
Below is a condensed version of the complete credentialing checklist template that Vigilant Medical Group uses for every provider enrollment. You can adapt this for any payer and any provider type.
Final Thoughts
Don't Let Credentialing Delays Cost You Revenue
- www.vigilantbillingms.us
- Fast. Accurate. Compliant.